




Guest Post: What evidence actually underlies blood pressure management? The Vast Overtreatment of Blood Pressure
The Vast Overtreatment of Blood Pressure
What evidence actually underlies blood pressure management?

-
High blood pressure (hypertension) is increasingly common, with more people diagnosed each decade.
-
At least 25% of hypertension diagnoses are due to inaccurate measurements.
-
The cause of hypertension is unknown for over 90% of patients.
-
Aggressively treating blood pressure is believed to prevent cardiovascular disease but only has a limited effect on strokes, not heart disease.
-
The correlation between high blood pressure and cardiovascular disease is often misinterpreted; impaired circulation causes blood pressure to rise, not the other way around.
-
In this article, I discuss the limitations of conventional blood pressure perspectives and explore the actual causes of high blood pressure (hypertension).
Ever since I first encountered the medical field, something struck me as off about their relentless focus on blood pressure. Before long, I noticed that the blood pressures the same acquaintances (e.g., relatives, patients, friends) shared with me varied immensely. While pondering this, a talented practitioner and mentor once told me that the current medical paradigm fixates on blood pressure because it's easier to measure than blood perfusion (healthy blood flow).
Then, as I became more acquainted with the medical field, I began to notice a consistent pattern—whenever a drug existed that could treat a number or statistic, as the years went by, the acceptable number kept on being narrowed, making more and more people eligible to take the drugs that treated the number.
For example, as I discussed recently, once the statins drugs entered the market (which unlike their predecessors, could effectively lower cholesterol), the acceptable blood cholesterol levels kept on being lowered, and before long almost everyone was told they would die from a heart attack unless they started a statin—despite statins have an almost non-existing mortality benefit (e.g., taking them for five years at best makes you live 3-4 days longer) and causing (often severe) side effects for roughly 20% of users. In turn, since so many people have been severely harmed by the great statin scam, more and more people, such as comedian Jimmy Dore have begun to speak out against this:
Broadly recommending these drugs hence appears unconscionable, but as I showed in that article, these unjustifiable guidelines were a product of clever pharmaceutical marketing and targeted bribery of public officials.
In today’s article, I will attempt to show how something similar happened with blood pressure management.
Conventional Blood Pressure Perspectives
Within the existing model, those consequences are:
•Weakened blood vessels become more likely to break open and leak as higher blood pressure pushes against them. This for instance, is why Emergency Rooms aggressively lower the blood pressure of patients who show up with symptoms of “hypertensive emergency,” such as a severe headache and a significantly elevated blood pressure. Likewise, whenever a critical blood vessel ruptures (e.g., the aorta or one in the brain), once the bleed has been confirmed, the first step in managing it is to lower the patient’s blood pressure (so less blood leaks out) after which they are sent to surgery.
•Excessive pressure on the arteries strains and damages them, causing the lining of the vessels to become damaged and gradually develop atherosclerosis.
•Excessive blood pressure damages the internal organs (termed end-organ damage), leading to premature failure and early death (e.g., from a heart attack or kidney failure).
Because of this, high blood pressure is viewed as one of the greatest preventable causes of cardiovascular disease, and thus, ensuring a patient achieves sufficiently lowered blood pressure is a chief focus of all medical visits.
Unfortunately, that chain of logic has quite a few holes in it.
Variable Blood Pressure
Measurement errors, like using the wrong cuff size or not accounting for differing BP in each arm, contribute to the issue. It's estimated that 25% of hypertension diagnoses are incorrect. Moreover, there is often a poor correlation between peripheral BP (limbs) and central BP (inside the aorta). Central BP, which is more closely linked to cardiovascular disease, can differ significantly from arm readings. Different BP medications also affect central and peripheral BP differently, adding complexity to treatment.
What Affects Blood Pressure?
Blood pressure is thus a product of two factors: the amount of blood in the arteries and the constriction or relaxation of the arteries containing it.
Note: since arterial BP is greater than venous BP, it’s what’s measured externally (as veins compress long before arteries do, and only arterial blood has a signature pulsatile wave created by the heartbeat).
Since each heartbeat pushes blood into the arteries and hence increases the pressure within them, two different blood pressure values exist—the baseline pressure (known as the diastolic pressure or DBP) and the pressure when the heart contracts (known as systolic pressure or SBP). The blood pressure values you see (e.g., 140/90) represent the maximum and minimum.
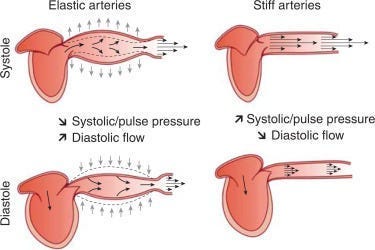
Note: one reason why this stretching is important is that when the vessels contract back to their normal size once the systolic pressure fades, that recoil pushes blood further along into the circulation.
Blood pressure lowering medications in turn work by some combination of:
-
Loosening the arterial walls
-
Reducing the total blood in circulation
-
Weakening the contraction of the heart
What Causes High Blood Pressure?
For the remaining 5-10% (known as secondary hypertension), recognized causes include reduced blood flow to the kidneys (which sets off a signal to raise the blood pressure because the kidney believes there isn’t enough blood perfusion), sleep apnea, or having a rare tumor that releases a blood pressure increasing hormone).
Since the cause of most hypertension is unclear, medicine focuses on risk factors like age, diabetes, salt intake, obesity, stress, and family history.
Note: effectively addressing anxiety can often cure a high blood pressure that would otherwise be perpetually medicated.
Atherosclerosis and Blood Pressure
Many of my colleagues became suspicious of the traditional blood pressure model after noticing that circulatory impairments often occurred alongside rising blood pressure, not as a result of long-term damage from it. This led us to conclude that elevated blood pressure might be a compensatory response to inadequate blood flow, similar to how the kidneys raise blood pressure when they don’t receive enough blood.
Several factors support this idea:
-
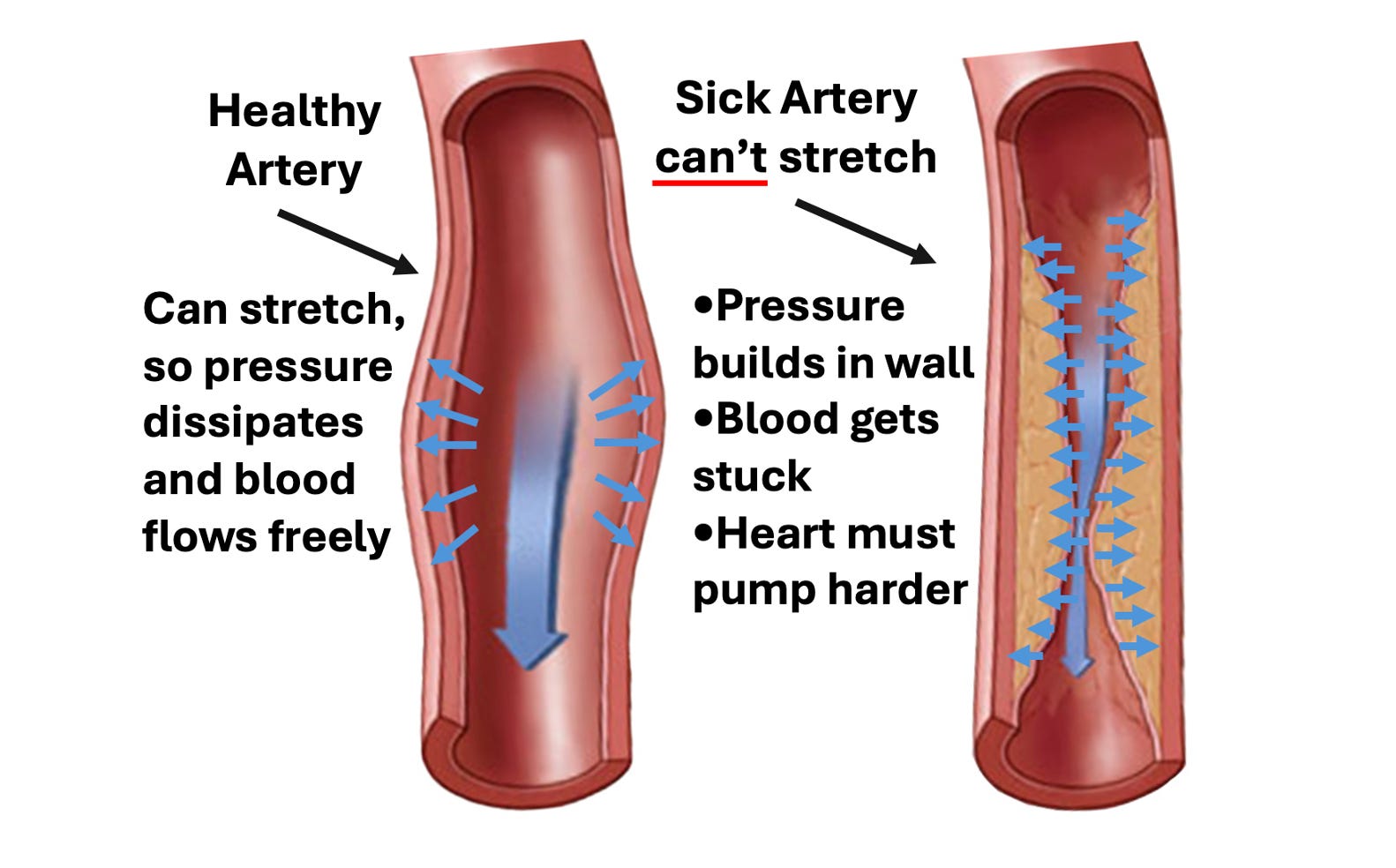
Arterial Stiffening: Calcified arteries can't expand as effectively, raising blood pressure as they become less able to release pressure.
-
Measurement Inaccuracy: Blood pressure cuffs may overestimate pressure in stiffened arteries, especially in those with severe atherosclerosis, leading to higher readings than the actual pressure (as the hardened arteries require more pressure to compress).
-
Endothelial Dysfunction: The blood vessel lining releases nitric oxide to dilate vessels and decrease pressure. When this function fails, it precedes atherosclerosis and increases blood pressure, suggesting the problem is with endothelial health, not high blood pressure itself.
-
Sympathetic Reflex: When the body rapidly loses a significant amount of blood, a reflex triggers increased heart rate and vessel constriction to raise blood pressure, a common response in critical conditions.
This all suggests that high blood pressure may be more of a symptom than the root cause of circulatory issues.
Zeta Potential and Blood Pressure
Zeta potential, a crucial component of health, quantifies the electrical charge difference between colloidal particles in a liquid. When sufficient zeta potential is present, those particles stay separated, while in disease states, they clump together. Many dangerous agents (e.g., aluminum, the spike protein, and the dangerous microbes) disrupt zeta potential, which commonly leads to blood cells in the body clumping together and microstrokes.
This process is recognized by many medical systems (e.g., Chinese medicine has the diagnosis blood stasis, which is almost identical to blood sludging, a concept many Western researchers previously demonstrated was a root cause of disease) and with appropriate examination can easily be detected (e.g., there are many neurological deficits frequently triggered by microstrokes which can be detected with the appropriate examination).
Sludged blood, in turn, can raise blood pressure by:
•Create a backlog in the circulation, which would increase the pressure on it (since blood would push against the arterial walls instead of being pushed forward).
•Signal the body to increase its blood pressure so the pockets of sludged blood could be pushed along.
•Directly stretch the smaller blood vessels, thereby increasing their pressure (and simultaneously “stiffen” the arteries because the clumps of sludge would have significantly more resistance to compression than dispersed blood cells).
To illustrate:
The blood sludging researchers repeatedly observed small arteries (e.g., those in the eyes) become stretched by larger sludges.
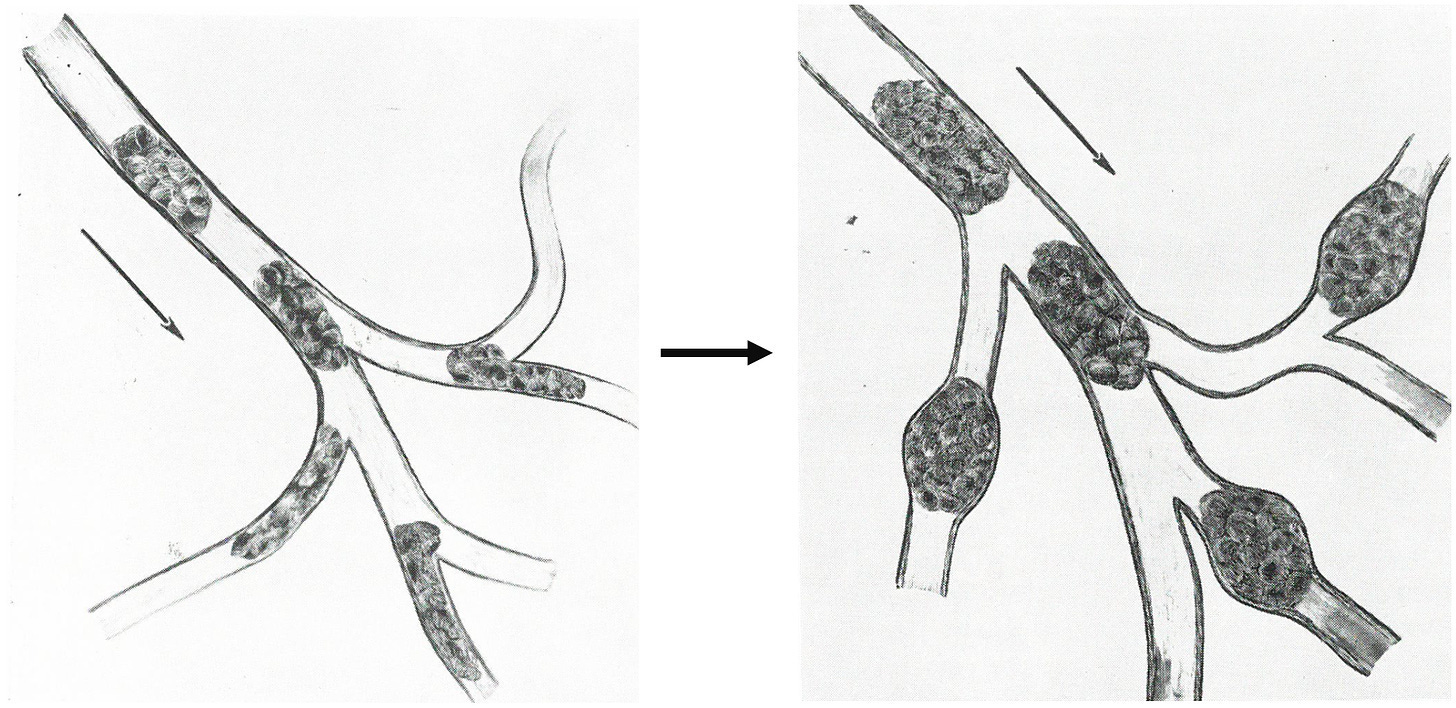
Additionally, they observed that once the pockets of sludge formed, the pressure build-up caused plasma (the non-cellular component of the blood) to begin leaking out into the tissues, leading to things like edema (swelling). Thus, the remaining blood became even more concentrated in these sludge pockets.
Note: once the zeta potential concept was applied to this phenomenon, it was noted that like other colloids, if their motion was slowed, blood cells would clump together and existing clumps would enlarge. This may in part explain why immobility and a lack of exercise are so detrimental to cardiovascular health.
While blood sludging primarily affects smaller vessels, causing microstroke-like injuries, it also impacts larger vessels by obstructing the vasa vasorum, the small blood vessels that nourish arteries. When the blood supply to the vasa vasorum is cut off, the endothelial lining of its artery dies, leading to high blood pressure and cardiovascular disease.
Note: motion breaks up these clumps, which may partly explain why immobility is linked to heart disease.
In turn, zeta potential researchers believed poor zeta potential was linked to atherosclerosis and found restoring zeta potential to be one of the most effective ways to normalize blood pressure (and treat heart disease).
A 2019 study supports this. It compared the zeta potential of 64 patients with hypertension to 50 controls....
Read more on A Midwestern Doctor's Substack here

